")
A new client came in this week for her first session with me. A few weeks ago, she was rear-ended in a car accident, and like most people who go through that kind of trauma, her body was still holding onto the impact. She booked a 60-minute session and told me her neck and shoulders were the main source of her pain.
That’s where she wanted me to work. But that’s not where I started.
Reading the Body Before Touching It
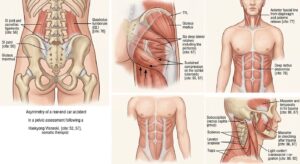
Before I put my hands on her, I did a quick SI joint and pelvic assessment. What I found told a bigger story than her chief complaint did: her right hip was internally rotated, her left hip was externally rotated, and her pelvis was sitting at a noticeable rotation.
Here’s the thing about car accidents — especially rear-end collisions. The force doesn’t just stay in your neck. It travels. The pelvis is the foundation of the spine, and when it twists or shifts from impact, the rest of the body compensates all the way up the chain. Tight neck? Cranky shoulders? Often, those are downstream symptoms of an upstream problem.
So even though her pain was up top, I knew I had to start at the bottom.
Building From the Foundation: Pelvis and Hips
I started by placing a body block under her right hip at the iliac crest, and another under her left hip at the acetabulum where the femoral head meets the pelvis. This positioning helps the pelvis gently reset while gravity does some of the work.
From there, I applied sustained compression on her right sit bone (ischial tuberosity) for about 60 seconds, then moved to her left side and held compression around the SI joint and iliac crest for another 60 seconds. Slow, sustained pressure — letting the tissue soften rather than forcing it.
Once she was settled in, I worked through the deeper hip layers: the gluteal group, the TFL, and the deep six lateral rotators (piriformis and friends). These muscles are notorious for hanging onto post-accident tension and pulling the pelvis out of alignment.
Moving Up the Spine
From the hips, I worked into the SI joint and lumbar region, paying special attention to the quadratus lumborum on both sides. The QL is one of those muscles that connects the pelvis to the ribcage, and when the pelvis is rotated, the QL is almost always part of the story.
Then I followed the erector spinae up both sides of the spine, working the long muscles that run from her sacrum all the way up to the base of her skull.
A Detour Through the Belly
Here’s where things got interesting. She told me she didn’t want me working on her legs — she wanted to stay focused on the upper body. Totally fair. But I still needed a way to release the legs, the deep hips, and even the shoulders and neck indirectly.
So I worked her abdomen — specifically the rectus abdominis. The anterior fascial line runs from the front of the thighs through the abdomen and up into the neck and jaw. Releasing the belly is one of the most underrated ways to unlock tension in places you’re not directly touching. It’s a beautiful workaround when a client wants targeted work but their body is asking for something more global.
Shoulders, Jaw, and Face
By the time I got to the area she originally wanted me to focus on, her body was already significantly more open. The work landed deeper because the foundation underneath had been addressed.
On the posterior neck, I worked the suboccipitals (the rectus capitis group at the base of the skull), the scalenes, the levator scapulae, and both upper and lower traps.
Then I moved to the front and sides — the first rib, the clavicles, the anterior, middle, and posterior scalenes, the SCM and surrounding anterior neck tissue. Whiplash injuries hit the front of the neck just as hard as the back, and people often forget that.
I worked through the jaw and face too: the orbicularis oris around the mouth, the masseters, and the temporalis muscles at the sides of the head. After a car accident, people clench. They brace. The jaw stores so much of that fight-or-flight response.
Finishing With Stillness: Craniosacral at the Neck
After all the deep, specific work, I ended the session with about 5 minutes of craniosacral therapy at the neck.
This is the part of the session that doesn’t look like much from the outside. Just hands, light contact, almost no movement. But this is where the nervous system finally lets go. After 55 minutes of telling the body, “we’re going to work on this,” craniosacral is the moment when I tell the body, “okay, you’re safe now. Integrate.”
For a client coming off the trauma of a car accident, this kind of quiet finish matters as much as any deep tissue work. The body needs to know the session is complete, and that it doesn’t have to brace anymore.
The Takeaway
Her chief complaint was neck and shoulder pain. But the real problem started in her pelvis and traveled up. If I had just worked her neck for 60 minutes, she would have felt better for a day or two — and then the same pattern would have pulled everything tight again.
Bodies tell stories. The job is to listen to the whole story, not just the loudest chapter.